
This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc.
Copyright © 2024 Med Learning Group. Built by Divigner. All Rights Reserved.
Treatments
Comprehensive treatment guidelines and information about specific agents for treating non-Hodgkin’s like chemotherapy, radiation, and immunotherapy, and their clinical trial data can be accessed in the Resources and CME Activities sections.
Treatments are broadly divided into the following five categories:
Chemotherapy
The most common course of non-Hodgkin’s chemotherapy is CHOP (cyclophosphamide, doxorubicin, prednisone, and vincristine), often with an addition of a monoclonal antibody, either rituximab (R-CHOP) or obinutuzumab (O-CHOP). Other non-Hodgkin’s chemotherapy regimens include a combination of bendamustine and rituximab, fludarabine, and R-CVP (rituximab, cyclophosphamide, prednisone, vincristine).2 Chemotherapy is sometimes used to prepare the patient for a bone marrow transplant/stem cell transplant.3
Radiation therapy3
Non-Hodgkin’s radiation therapy utilizes high-energy beams such as X-rays or protons to destroy cancer cells. Radiation treatments for non-Hodgkin’s lymphoma can be used alone to destroy one or two targeted spots that contain cancerous lymphoma and can be used post-chemotherapy to destroy any lymphoma cells that remain.
Immunotherapy2
Non-Hodgkin’s immunotherapy treatments boost the patient’s own immune system to fight cancer. This includes the use of modified T cells and checkpoint inhibitors. In chimeric antigen receptor (CAR) T cell therapy (CAR T) some of the patient’s own T cells are removed and modified to contain specific proteins called receptors. The receptors allow these modified T cells to recognize cancer cells that have the target protein that binds to these receptors. These modified T cells are grown in a lab and then returned to the patient’s body.
Currently available FDA-approved CAR T non-Hodgkin’s immunotherapy options include axicabtagene ciloleucel, tisagenlecleucel, brexucabtagene autoleucel, and lisocabtagene maraleucel.
Immune checkpoint inhibitor: pembrolizumab
Targeted therapy2
- Anti-CD20 Monoclonal antibodies (mAbs): rituximab, obinutuzumab, and ofatumumab
- Anti-CD20 Radiolabeled antibodies: ibritumomab tiuxetan
- Antibody-drug conjugates (ADCs): brentuximab (CD30), loncastuximab tesirine-lpyl (CD19), polatuzumab vedotin-piiq (CD79b), tafasitamab-cxix (CD19)
Other targeted FDA-approved therapies for the treatment of NHL include:
- Bruton’s tyrosine kinase (BTK) inhibitors: ibrutinib, acalabrutinib, and zanubrutinib
- BCL-2 inhibitor: venetoclax
- PI3 kinase inhibitors: copanilisib, idelalisib, and duvelisib
- Selective inhibitor of nuclear export (SINE): selinexor
- Immunomodulatory drug: lenalidomide
- Enhancer of zeste homolog 2 (EZH2) inhibitor: tazemetostat
- Histone deacetylase (HDAC) inhibitors: belinostat, romidepsin, and vorinostat
- Proteasome inhibitor: and bortezomib1
Bone Marrow Transplant2,4
This involves using high doses of radiation and chemotherapy to suppress the patient’s bone marrow and immune system. Transplants are either autologous (patient’s own stem cells) or allogenic (donor stem cells).
Further details on each of these therapies can be accessed in the Resources section.
First-line Treatment
First-line treatment for most kinds of NHL is RCHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). Other recommended regimens include dose-adjusted EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin) + rituximab.
Diffuse large B-cell lymphoma
Figure 1 is an example of the treatment landscape for DLBCL. Similar information on treatments for each type of NHL can be explored in the CME activities section. Presenting symptoms include rapidly enlarging masses with both local and systemic symptoms (B symptoms with fever, night sweats, and weight loss).
Most patients with localized tumors can be cured with chemotherapy for non-Hodgkin’s alone or in combination with immunomodulatory agents. For advanced disease, more than half the patients are cured by doxorubicin-based combination therapy and rituximab.9
Figure 1: Current treatment landscape for DLBCL1
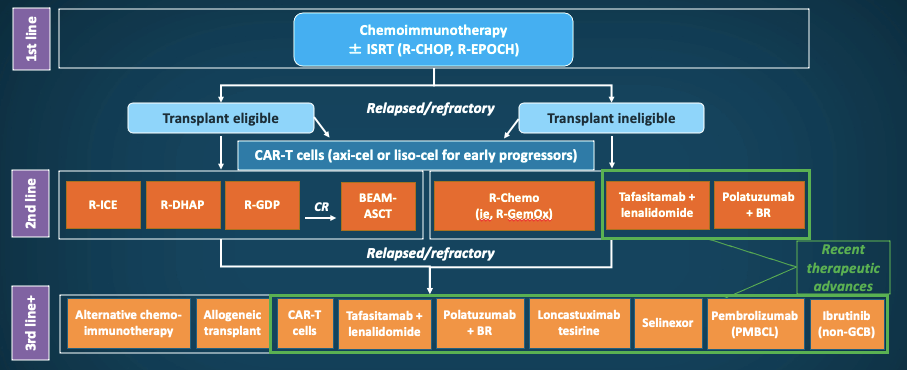
ASCT = autologous stem cell transplantation; axi-cel = axicabtagene ciloleucel; BEAM = carmustine, etoposide, cytarabine, and melphalan; BR = bendamustine and R; CAR-T = chimeric antigen receptor on T cell; CR = complete response; GCB = germinal center B-cell; ISRT = involved-site radiation therapy; liso-cel = lisocabtagene maraleucel; PMBCL = primary mediastinal large B-cell lymphoma; R = rituximab; R-Chemo = R and chemotherapy; R-CHOP = R, cyclophosphamide, doxorubicin, vincristine, and prednisone; R-DHAP = R, dexamethasone, cytarabine, and cisplatin; R-EPOCH = R, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin; R-GDP = R, gemcitabine, cisplatin, and dexamethasone; R-GemOx = R, gemcitabine, and oxaliplatin; R-ICE = R, ifosfamide, carboplatin, and etoposide.
Table 1: Treatment for R/R DLBCL1
| Second-line therapy (intention to proceed to transplant | |
|---|---|
|
Preferred regimens (alphabetical order)
|
Other recommended regimens (alphabetical order)
|
| Second-line therapy (non-candidates for transplant) | |||
|---|---|---|---|
|
Preferred regimens (alphabetical order):
|
Other recommended regimens (alphabetical order):
|
Useful in certain circumstances:
|
Anti-CD19 CAR T-cell therapy:
|
| Third-line and subsequent therapy | |
|---|---|
|
Anti-CD19 CAR T-cell therapy |
Axicabtagene ciloleucel |
|
Antibody-drug conjugate (ADC) |
Loncastuximab tesirine-lpyl |
|
Selective inhibitor of nuclear export (SINE) |
Selinexor |
Follicular lymphoma
Follicular lymphoma is a tumor containing follicle center cells, a combination of centrocytes and centroblasts.5 As it is an indolent tumor, median survival ranges from 8-15 years. Watchful waiting and deferment of treatment till the patient has symptoms is an option in patients with advanced FL and remains a standard of care.6 Rituximab alone or in combination with various chemotherapeutic drugs or in combination with immunomodulating agents (eg, lenalidomide) is a therapeutic option. PI3K inhibitors have been known to be effective in R/R disease.7 Autologous or allogeneic stem cell transplant may also be considered as consolidation therapy for relapsed disease. Table 2 outlines various therapeutic options for R/R FL.
Patients with indolent lymphomas may have a more aggressive histology when undergoing a relapse, and a biopsy at this stage can help make an appropriate change to the therapy applicable to that histologic state.8
Table 2: Treatment for R/R FL1
| Second-line therapy | |
|---|---|
|
Preferred regimens (alphabetical order):
|
Other recommended regimens (alphabetical order):
|
| Third-line and subsequent therapy | |
|---|---|
|
PI3K inhibitors |
Copanlisib |
|
EZH2 inhibitors |
Tazemetostat |
|
Anti-CD19 CAR T-cell therapy |
Axicabtagene ciloleucel Tisagenlecleucel |
Table 3: Treatment for R/R Mantle cell lymphoma1
| Second-line and subsequent therapy | |
|---|---|
|
Preferred regimens (alphabetical order):
|
Useful in certain circumstances (alphabetical order):
|
|
Second-line consolidation |
|
|
Allogenic hematopoietic cell transplant in selected cases |
|
|
Third-line therapy |
|
|
Brexucabtagene autoleucel (only after chemoimmunotherapy and BTK inhibitor) |
|
Some novel treatment approaches for mantle cell lymphoma are described in Table 4.
Table 4: Novel treatments for R/R mantle cell lymphoma
| Agent | N | ORR, % | CR, % | mDOR, mos |
|---|---|---|---|---|
|
Bortezomib10 |
155 |
32 |
8 |
9.2 |
|
Lenalidomide10 |
134 |
28 |
7.5 |
16.6 |
|
Lenalidomide-rituximab14 |
52 |
57 |
36 |
18.9 |
|
Ibrutinib13 |
370 |
69.7 |
27 |
21.8 |
|
Acalabrutinib14 |
124 |
81 |
43 |
26 |
|
Zanubrutinib15 |
32 |
84 |
25 |
18.5 |
|
Venetoclax16 |
20 |
53 |
18 |
8.1 |
|
Ibrutinib-venetoclax17 |
24 |
71 |
62 |
NR; 78% PFS at 15 mos. |
|
Obinutuzumab-ibrutinib-venetoclax18 |
48 |
79 |
67 |
NR; 74.5% PFS at 12mos. |
References
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 5.2022. Updated July 12, 2022. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf
- Cancer.Net. Lymphoma – Non-Hodgkin: Types of Treatment. Approved March 2021. https://www.cancer.net/cancer-types/lymphoma-non-hodgkin/types-treatment
- Mayo Clinic. Non-Hodgkin’s lymphoma. Diagnosis and Treatment. May 4, 2021. https://www.mayoclinic.org/diseases-conditions/non-hodgkins-lymphoma/diagnosis-treatment/drc-20375685
- Lymphoma Research Foundation. Understanding Non-Hodgkin’s lymphoma. 8th ed; Fall 2020. https://lymphoma.org/wp-content/uploads/2021/04/LRF-NHL-Booklet_4.21.pdf
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: A review. J Family Med Prim Care. 2020;9:1834-1840. https://doi.org/10.4103/jfmpc.jfmpc_1037_19
- Armitage JO, Longo DL. Is watch and wait still acceptable for patients with low-grade follicular lymphoma? Blood. 2016;127:2804-2808. https://doi.org/10.1182/blood-2015-11-632745
- Dreyling M, Santoro A, Mollica L, et al. Phosphatidylinositol 3-kinase inhibition by copanlisib in relapsed or refractory indolent lymphoma. J Clin Oncol. 2017;35:3898-3905. https://doi.org/10.1200/JCO.2017.75.4648
- Tsimberidou AM, O’Brien S, Khouri I, et al. Clinical outcomes and prognostic factors in patients with Richter’s syndrome treated with chemotherapy or chemoimmunotherapy with or without stem-cell transplantation. J Clin Oncol. 2006;24:2343-2451. https://doi.org/10.1200/JCO.2005.05.0187
- PDQ Adult Treatment Editorial Board. Adult Non-Hodgkin’s Lymphoma Treatment (PDQ®): Health Professional Version. In: PDQ Cancer Information Summaries. National Cancer Institute. July 6, 2022. https://www.ncbi.nlm.nih.gov/books/NBK66057/
- Goy A, Bernstein SH, Kahl BS, et al. Bortezomib in patients with relapsed or refractory mantle cell lymphoma: Updated time-to-event analyses of the multicenter phase 2 PINNACLE study. Ann Oncol. 2009;20:520-525. https://doi.org/10.1093/annonc/mdn656
- Goy A, Sinha R, Williams ME, et al. Single-agent lenalidomide in patients with mantle cell lymphoma who relapsed or progressed after or were refractory to bortezomib: Phase II MCL-001 (EMERGE) study. J Clin Oncol. 2013;31:3688-3695. https://doi.org/10.1200/JCO.2013.49.2835
- Wang M, Fayad L, Wagner-Bartak N, et al. Lenalidomide in combination with rituximab for patients with relapsed or refractory mantle cell lymphoma: A phase 1/2 clinical trial. Lancet Oncol. 2012;13:716-723. https://doi.org/10.1016/S1470-2045(12)70200-0
- Rule S, Dreyling M, Goy A, et al. Ibrutinib for the treatment of relapsed/refractory mantle cell lymphoma: Extended 3.5-year follow up from a pooled analysis. 2019;104:e211-e214. https://doi.org/10.3324/haematol.2018.205229
- Wang M, Rule S, Zinzani PL, et al. Durable response with single-agent acalabrutinib in patients with relapsed or refractory mantle cell lymphoma. 2019;33:2762-2766. https://doi.org/10.1038/s41375-019-0575-9
- Tam CS, Opat S, Simpson D, et al. Zanubrutinib for the treatment of relapsed or refractory mantle cell lymphoma. Blood Adv. 2021;5:2577-2585. https://doi.org/10.1182/bloodadvances.2020004074
- Eyre TA, Walter HS, Iyengar S, et al. Efficacy of venetoclax monotherapy in patients with relapsed, refractory mantle cell lymphoma after Bruton tyrosine kinase inhibitor therapy. 2019;104:e68-e71. https://doi.org/10.3324/haematol.2018.198812
- Tam CS, Anderson MA, Pott C, et al. Ibrutinib plus venetoclax for the treatment of mantle cell lymphoma. N Engl J Med. 2018;378:1211-1223. https://doi.org/10.1056/NEJMoa1715519
- Le Gouill S, Morschhauser F, Chiron D, et al. Ibrutinib, obinutuzumab, and venetoclax in relapsed and untreated patients with mantle cell lymphoma: a phase 1/2 trial. 2021;137:877-887. https://doi.org/10.1182/blood.2020008727
