For all B-cell lymphomas, diagnosis is confirmed via excisional or incisional biopsy, and a fine needle aspiration (FNA) biopsy on its own is not considered suitable for initial non-Hodgkin’s lymphoma diagnosis. A combination of core needle biopsy (preferably multiple biopsies) and FNA biopsies in conjunction with other techniques such as immunohistochemistry (IHC), flow cytometry, and molecular analysis for the detection of immunoglobulin gene rearrangements, karyotype, or FISH for major translocations) may be sufficient for a non-Hodgkin’s lymphoma diagnosis. Additionally, a hematopathology review of all slides with at least one paraffin block representative of the tumor is required.2Additional diagnostic blood tests and exams for non-Hodgkin’s lymphoma, focusing on each unique type, may be required and information about these can be found in the Resources section.
Non-Hodgkin’s Lymphoma Staging
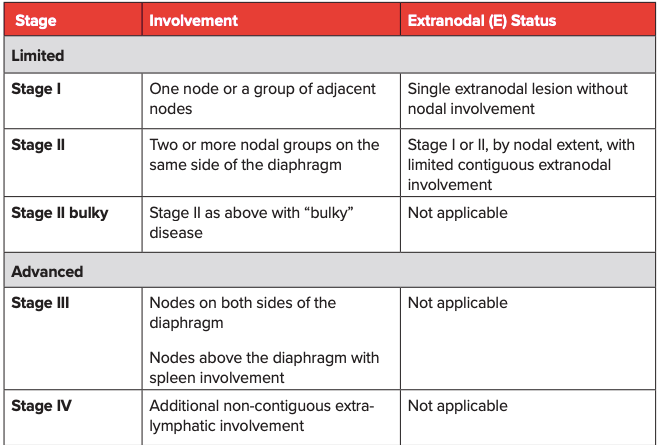
Non-Hodgkin’s lymphoma staging is a way to determine where the cancer is, and how much it has spread to other sites. A thorough staging will help determine the best course of treatment.3Non-Hodgkin’s lymphoma staging is typically carried out according to the Ann Arbor classification system (Table 1), with a mention of bulky disease when that is applicable. For follicular lymphoma (FL), an FL International Prognostic Index or FLIPI that considers nodal sites (>4 lymph nodes), age (>60 years), serum marker (elevated LDH), stage of disease (advanced Ann Arbor classification stage III-IV), and hemoglobin to categorize patients into low risk (0-1 risk factor), intermediate risk (2 risk factors), and high risk (3-5 risk factors) has been established. For patients requiring treatment, a revised FLIPI2 score that incorporates beta-2-microglobulin, the diameter of the largest lymph node, bone marrow involvement, and hemoglobin levels is available.3
Table 1: Lugano modification of the Ann Arbor Staging System (for primary nodal lymphomas)1
References
Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging and response assessment of Hodgkin and non-Hodgkin’s lymphoma: The Lugano classification. J Clin Oncol. 2014;32:3059-3067. https://doi.org/10.1200/JCO.2013.54.8800
Dreyling M, Ghielmini M, Rule S, et al. Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32:298-308. https://doi.org/10.1016/j.annonc.2020.11.008