Pathogenesis
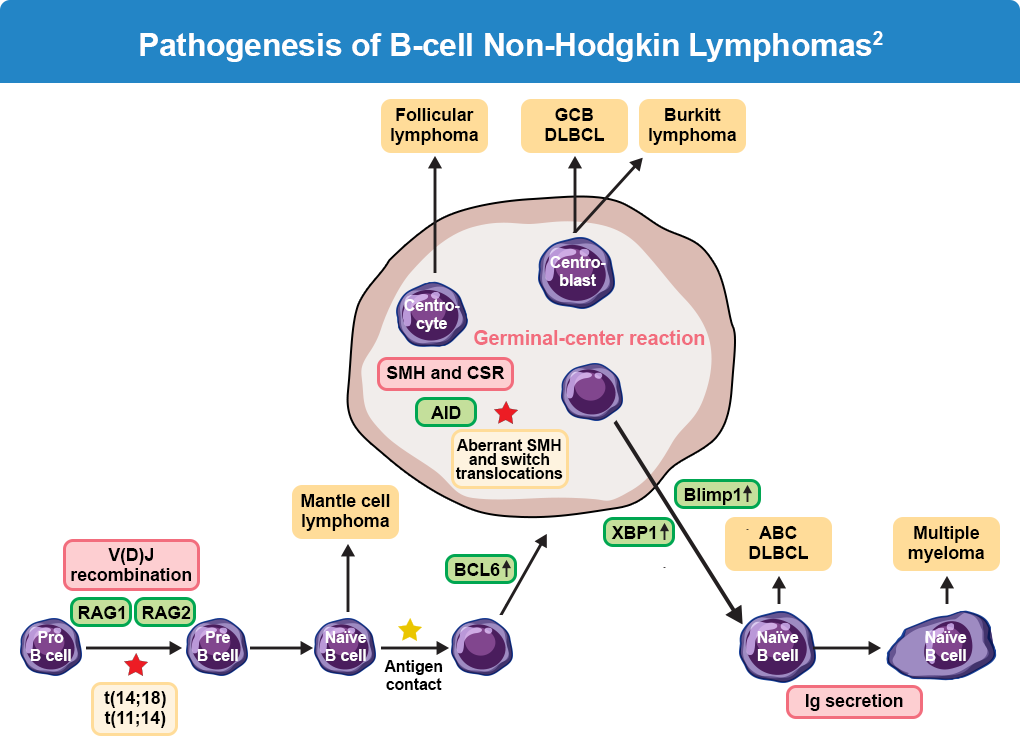
Most NHL cancers are associated with chromosomal abnormalities, originating within a single cell, with subsequent cells carrying the identical variation.1 As such, lymphomas arise at different stages of B-cell differentiation. Specific recombination events lead to the development of chromosomal aberrations. The germinal center is surrounded by a mantle zone of naive B cells, most of which express the CD5 marker, which might comprise a distinct B-cell subset. Recombination activating gene 1 (RAG1)-dependent and RAG2-dependent V(D)J recombination takes place in the bone marrow. The potentially resulting t(14;18) and t(11;14) represent critical first steps in lymphomagenesis of different lymphoma subtypes. After antigen contact, the stimulated B cells migrate to the lymph node and form the germinal center after upregulation of BCL6. The events during the germinal center reaction include activation-induced cytidine deaminase (AID)–mediated somatic hypermutation and class-switch recombination, which are critical events for lymphoma evolution. The germinal center reaction is terminated by the differentiation of B cells into plasma cells. XBP1 and Blimp-1 are key regulators for plasmacytic differentiation.1-3
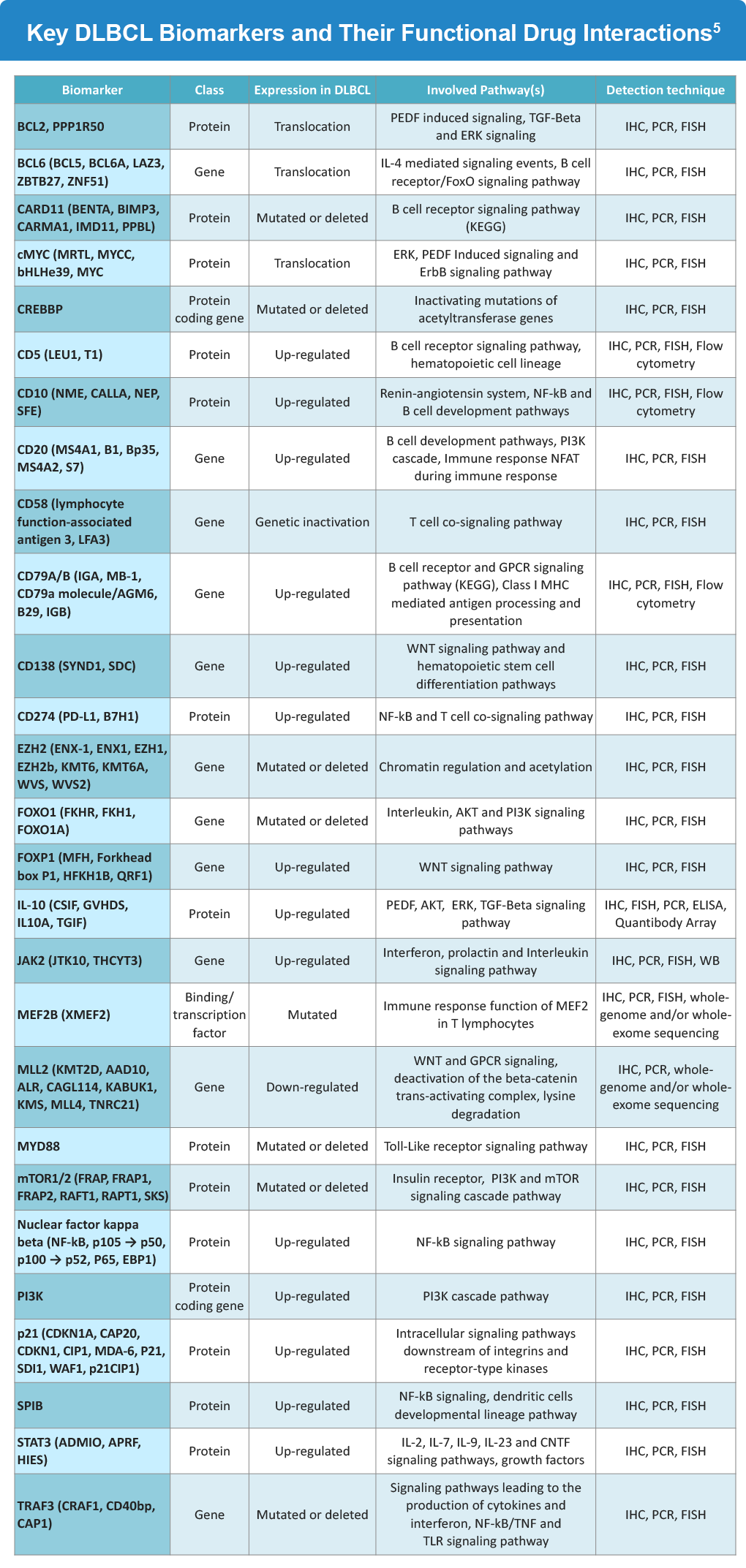
Various recurrent genomic and molecular biomarkers are involved in B-cell lymphomas, with prognostic effects related to various genetic abnormalities in proteins including MYC, BCL2, BCL6, TP53, etc.1 Additionally, development of unique anti-CD antibodies for treatment of specific lymphomas is possible due to specific biomarker expression at each stage of B-cell development and differentiation.

Taking CD20 expression as an example, it is largely restricted to B-cells and certain stages of their development; pro-B cells, differentiated plasmablasts, or plasma cells do not express CD20. Furthermore, CD20 is detected in approximately 95% of all B-cell malignancies.4 Key biomarkers implicated in DLBCL, including their expression patterns, associated signaling pathways, and common detection techniques, are summarized below.
References
- Sun R, Medeiros LJ, Young KH. Diagnostic and predictive markers for lymphoma diagnosis and treatment in the era of precision medicine. Mod Pathol. 2016;29:1118-1142. doi:10.1038/modpathol.2016.92
- Nogai H, Dörken B, Lenz G. Pathogenesis of non-Hodgkin’s lymphoma. J Clin Oncol. 2011;29:1803-1811. doi:10.1200/JCO.2010.33.3252
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 3.2026. March 12, 2026. (https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf)
- Forsthuber TG, Cimbora DM, Ratchford JN, Katz E, Stüve O. B cell-based therapies in CNS autoimmunity: Differentiating CD19 and CD20 as therapeutic targets. Ther Adv Neurol Disord. 2018;11:1756286418761697. doi:10.1177/1756286418761697
- Lodhi N, Tun M, Nagpal P, et al. Biomarkers and novel therapeutic approaches for diffuse large B-cell lymphoma in the era of precision medicine. Oncotarget. 2020;11:4045-4073. doi:10.18632/oncotarget.27785
ALL URLs accessed April 27, 2026
