Treating & Managing NHL
A summary of treatment guidelines for NHL, including diffuse large B-cell lymphoma (DLBCL), follicular lymphoma (FL) and mantle cell lymphoma can be found in the dedicated guideline recommendations section of the portal.
When to Refer
Refer all patients with suspected lymphoma to a clinical hematologist, medical oncologist, or general physician (ie, in regional/rural areas) who works in association with a multidisciplinary team and has appropriate expertise in the management of lymphoma. Often, lymphoma workup, diagnosis, specialist referral, and treatment planning can all be completed in the outpatient setting. However, high grade lymphomas, such as Burkitt lymphoma, certain subsets of diffuse large B-cell lymphoma, lymphoblastic lymphoma, some mantle cell lymphomas, and peripheral T- and NK-cell lymphomas are associated with a high tumor proliferation rate and extensive disease burden that can result in medical emergencies. Prompt recognition of this subset is vital as medical emergencies related to aggressive lymphoma confer a worse prognosis. Recognition of potential emergencies by the generalist is important as they may be present during initial evaluation, necessitating hospitalization and immediate hematology/oncology consultation for intervention and expedited treatment.1,2
Treatment
Treatments for NHL are broadly divided into the following five categories:3
Chemotherapy
The most common regimen of chemotherapy is CHOP (cyclophosphamide, doxorubicin, prednisone, and vincristine), often with an addition of a monoclonal antibody, either rituximab (R-CHOP) or obinutuzumab (O-CHOP). Other chemotherapy regimens include a combination with bendamustine and rituximab, fludarabine, and R-CVP (rituximab, cyclophosphamide, prednisone, vincristine).4 Recently, Pola-R-CHP, a modified drug combination that switches vincristine for polatuzumab vedotin has been approved for patients with previously untreated diffuse large B-cell lymphoma (DLBCL), not otherwise specified (NOS), or high-grade B-cell lymphoma (HGBL) and an International Prognostic Index of ≥2 and has shown a significantly superior progression-free survival compared to R-CHOP treatment.5 Chemotherapy is sometimes used to prepare the patient for a bone marrow transplant/stem cell transplant.6
Radiation therapy
Radiation therapy uses high-energy beams (eg, X-rays or protons) to eradicate malignant cells. It may be employed as definitive treatment for localized disease or as consolidation following chemotherapy to eliminate residual lymphoma.5
Immunotherapy
Immunotherapy boosts the patient’s own immune system to fight cancer. This includes the use of modified T cells and checkpoint inhibitors. Chimeric antigen receptor (CAR) T-cell therapy involves harvesting autologous T cells, genetically engineering them to express tumor-specific receptors, expanding them ex vivo, and reinfusing them into the patient to target lymphoma cells. An immune checkpoint inhibitor binds to PD-1 or PD-L1 receptors located on the surface of the lymphoma cell preventing it from evading the body’s immune response.4,6
Currently available FDA-approved CAR T therapies include axicabtagene ciloleucel, tisagenlecleucel, brexucabtagene autoleucel, and lisocabtagene maraleucel. Similarly, approved immune checkpoint inhibitors include pembrolizumab and nivolumab.4,6
Targeted therapy
Targeted therapies act against a specific component within the molecular pathway involved in tumorigenesis. Several targeted therapies are currently approved by the FDA.4
- Anti-CD20 Monoclonal antibodies (mAbs): rituximab, obinutuzumab, and ofatumumab4
- Anti-CD19 mAb: tafasitamab-cxix4
- Antibody-drug conjugates (ADCs): brentuximab vedotin (CD30), loncastuximab tesirine-lpyl (CD19), polatuzumab vedotin-piiq (CD79b)
- Bispecific antibodies: glofitamab, epcoritamab (approved for DLBCL), mosunetuzumab (approved for FL), odronextamab (currently approved for use in the European Union to treat adult patients with relapsed or refractory (R/R) FL or R/R DLBCL, after two or more lines of systemic therapy; odronextamab is also in late-stage clinical development for use in both FL and DLBCL in the United States)4,7
Bispecific antibodies (BsAbs) are novel targeted therapies that are revolutionizing the treatment landscape of B cell NHL. In the relapsed/refractory setting, salvage chemotherapy and autologous stem cell transplantation show favorable outcomes in ~50% of patients, whereas the other half will have a poorer outcome with a median overall survival (OS) of less than 12 months. This unmet need reinforces the importance of innovative therapies like BsAbs.8-10

BsAbs are dual-targeted, antibody-based molecules that simultaneously bind a tumor-associated antigen and an immune effector cell, most commonly CD3 on T cells, thereby redirecting T cells to induce targeted tumor cell cytotoxicity. The clinical use of T-cell engaging antibodies in B-cell neoplasms began with the use of blinatumomab (an anti-CD19 BsAb) in acute lymphoblastic leukemia. More recently, the US FDA approved glofitamab for adults with R/R DLBCL, epcoritamab for R/R DLBCL and for R/R FL, and mosunetuzumab for R/R FL after two or more prior therapies.9,10
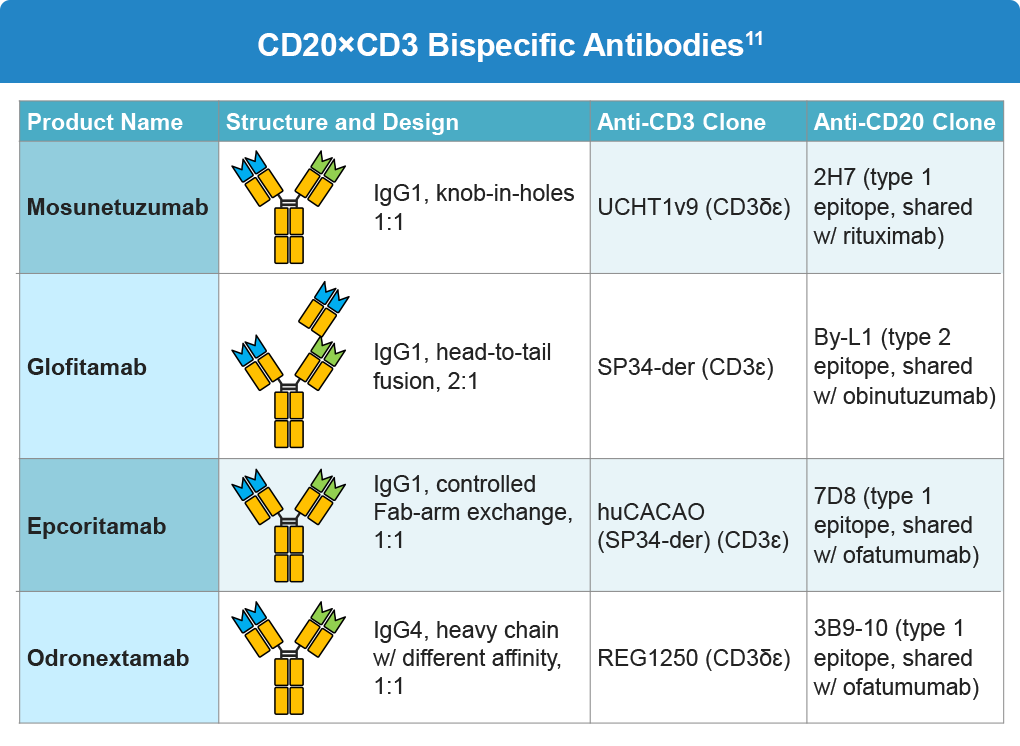
Mosunetuzumab
Mosunetuzumab is a full-length, humanized, immunoglobulin G1-based BsAb targeting CD20 on B-cells and CD3 on T-cells. A multicenter, single-arm phase II pivotal trial (NCT02500407) studied the efficacy of mosunetuzumab in 90 fit adult patients with R/R FL (grade 1–3a), after at least two prior lines of treatment, including an anti-CD20 therapy and an alkylating agent. The study demonstrated a reduction in tumor size in 95% of patients after a median follow-up of 18.3 months. The objective response rate (ORR) and complete response (CR) rates were 80% and 60%, respectively, and 70% of complete responders maintained response for at least 18 months. The observed CR rate was significantly higher (P <.0001) than the historical control CR rate of 14% reported with copanlisib therapy, thereby meeting the primary study endpoint. These data led to the regulatory approval in 2022 of mosunetuzumab for patients with R/R FL after ≥2 prior lines of therapy.8 An updated result of this pivotal phase II study after a median follow-up of 37.4 months showed that mosunetuzumab was associated with a CR rate of 60%, ORR of 77.8%, estimated 36-month overall survival (OS) rate of 82.4% (95% CI, 73.8-91.0) and progression-free survival (PFS) of 24 months (95% CI, 12.0 to NE). Median OS was not reached (95% CI, NE-NE).9
Another phase II trial was conducted among 230 patients with R/R B-cell NHL who were treated at different dose levels. The most common reported adverse events (AEs) were neutropenia (28%), cytokine release syndrome (CRS) (27%), hypophosphatemia (23%), fatigue (23%), and diarrhea (22%). Most AEs were of low grade, transient, and occurred early in the first cycle. Among 129 evaluable patients with aggressive B-NHL, the ORR was 34.9% and the CR rate was 19.4% with a median duration of response (DOR) of 22.8 months in complete responders. Patients with indolent NHL had longer median PFS of 11.8 months versus 1.4 months for aggressive NHL. The clinical response was strongly associated with mosunetuzumab exposure. Overall, mosunetuzumab has a favorable safety profile and can be administered in an outpatient setting.10
Glofitamab
Glofitamab is another potent anti-CD20-directed T-cell engager with a 2:1 molecular format to increase biological efficacy. This CD20xCD3 BsAb has the capacity to induce a 40-fold increase in lysis by high-avidity bivalent anti-CD20 and head-to-tail orientation of B- and T-cell binding domains as opposed to a classical 1:1 BsAb format. In a first-in-human phase I trial, glofitamab was administered in dose-escalation steps (0.005–30 mg) to 174 patients with R/R B-cell NHL. The participants were heavily pre-treated with a median of three prior therapies, and 90.6% were refractory to their last therapy. The study reported significant clinical activity starting at a dose level of 0.6 mg. Almost all patients had CRS at a dose level of 25 mg and this was considered as the maximum tolerated D1 dosing. Subsequently, the recommended phase II dose followed the step-up dosing (SUD) of 2.5 mg (C1D1), 10 mg (C1D8) and 30 mg (C2D1). The ORR and CR rates were 53.8% and 36.8%, respectively, in all dosed patients. The responses were higher (ORR: 65.7%, CR: 57.1%) among those who received the recommended phase II dose. Most responses occurred early during treatment, increasing substantially with dose escalation, with sustained responses in 84% of patients after a maximum observation period of 27.4 months. In part 2 of this phase II study, 39% of patients achieved a CR after a median of 42 days after a median follow-up of 12.6 months, which coincides with the first response assessment. Responses were seen across subgroups regardless of age, histology, and prior use of CAR T-cell therapy. Notably, while refractory patients presented a lower CR rate (34%) compared to non-refractory patients (70%), the response displayed remarkable durability, with 78% of responders maintaining their response at 12 months.9 In an updated landmark analysis with median follow-up of 37.7 months, the median-PFS and OS were 31.1 months (95% CI, 23.8–NE) and 44.8 months (95% CI, 40.0–NE), respectively.10 The most common AE was CRS, which occurred in 50.3% of all dosed patients, and in 71.4% of patients receiving recommended dosing of 2.5/10/30 mg; most incidents of CRS were grade 1 or 2: 25.1% and 22.9%, respectively.8
Epcoritamab
Epcoritamab is a CD20×CD3 BsAb that is administered subcutaneously with initial step-up dosing (SUD) and continued until disease progression. The dose escalation trial across all B-cell NHL subtypes escalated doses ranging from 0.0128 mg to 60 mg of single-agent epcoritamab in 68 highly refractory CD20+ mature B-cell NHL patients. The trial did not report any dose-limiting toxicities, and 48 mg was selected as the recommended phase II dose, as no additional responses were recorded beyond this dose. Most common AEs were CRS in 59% of patients (all grade 1 and 2) and injection-site reactions in 47%.8 Treatment with epcoritamab demonstrated ORR and CR rates of 68% and 45% in R/R DLBCL and 90% and 50% in R/R FL, respectively. In the dose-expansion cohort of the phase I/II trial, 157 patients with R/R mature B-cell NHL received a median of five cycles (15 doses) at the full dose of 48 mg after SUD (0.16 mg on D1 and 0.8 mg on D8). The ORR and CR rates were 63.1% and 38.9%, respectively. The median time to CR was 2.7 months (range, 1.2–11.1), with an estimated DOR of 12 months. The 6-month PFS rate was 44%; longer follow-up is needed to determine whether the PFS curve will reach a “plateau”. Epcoritamab demonstrated consistent responses across several pre-specified subgroups, including age, line of therapy, primary refractory disease, and prior exposure to CAR T-cell therapy. The safety profile was as expected from the initial reports of this trial, with the most common AEs being CRS, injection-site reactions, and neutropenia.8
Odronextamab
Odronextamab is an IgG-like CD20xCD3 BsAb, studied in the ELM trials for the treatment of various B-cell malignancies, including DLBCL and FL. ELM-1, a large dose-finding phase 1 study with FL=40, MCL=12, and marginal zone lymphoma (MZL)=6, reported ORRs of 91%, 50%, and 67% in FL, MCL, and MZL, respectively. The CR rates were 72%, 33%, and 33%, respectively. The dose for phase-2 FL was determined to be 80 mg. In long-term follow-up of ELM-2 (median follow-up, 34.1 months; n= 128), odronextamab demonstrated an ORR of 80.5% and a CR rate of 74.2% in patients with R/R FL who received 2 or more prior lines of therapy. Results from the Phase 3 OLYMPIA-1 trial investigating odronextamab monotherapy vs standard chemo-immunotherapy for heavily pretreated R/R FL (n=13, Part 1, with efficacy evaluable in 5/13 at week 12) demonstrated ORR and CR rates of 100% with no new safety signals identified. Step-up dosing for odronextamab was utilized for Part 1; Part 2 of the OYLMPIA-1 trial will continue to evaluate odronextamab at 80 mg dosing.12-14 In addition, odronextamab is being evaluated in combination with chemotherapy (CHOP/CVP), followed by odronextamab maintenance therapy, in previously untreated FL in the phase 3 OLYMPIA-2 study. In results in Part 1 of the study, among 16 evaluable patients, the ORR was 88.9% for DL1 and 100% for DL2. CR rates were 77.8% and 85.7%, respectively. The safety profile of odronextamab plus CHOP/CVP was generally manageable, with no new safety signals. The most common grade ≥3 TEAEs were neutropenia and anemia. Infections were frequent, with 7 patients requiring hospitalization. CRS was limited to grade 1/2 and no tumor lysis syndrome, ICANS, or treatment-emergent deaths were reported.15
In the DLBCL cohort of ELM-2, after a median follow-up of 29.9 months, results in 127 patients showed a CR and ORR of 31.5% and 52%, respectively. Odronextamab showed efficacy across several key subgroups, including patients who were >75 years of age (ORR, 50%), had >2 previous lines of therapy (ORR, 46.7%), or were refractory to both alkylator and anti-CD20 antibody therapy (ORR = 40.2%).16 Of 60 patients in the ELM-1 trial with R/R DLBCL after treatment with CAR-T cell therapy, the ORR and CR rates were 48.7% and 31.7%, respectively, after median follow-up of 16.2 months.17
Pooled data from long-term efficacy studies of odronextamab (ELM-1 and ELM-2, n=127) for R/R DLBCL in the third-line and later setting included 32.1% (n=60) of pooled participants that had received prior CAR-T cell therapy (29/60 with relapse within ≤90 days, 43/60 with CAR-T–refractory disease). Durable responses were noted, with noted ORR (50.8%) and CR (31.6%) rates being consistent across subgroups, including the post–CAR-T subgroup. Additionally, the median duration of CR was 36.3 months (95% CI, 12.4-NE), with a 51% probability of maintaining CR for 3 years.18 Similar to FL, odronextamab is being evaluated in combination with CHOP induction therapy in previously untreated CD20+ DLBCL. Part 1 results of the phase 3 open-label OLYMPIA-3 trial demonstrated encouraging efficacy, with ORRs of 77.8% for DL1 and 100% for DL2. CR rates were 66.7% and 100%, respectively, among 20 evaluable patients. Grade ≥3 TEAEs were reported in all patients, most commonly neutropenia. Infections were reported in 66.7% and 92.3% of patients at DL1 and DL2, respectively (grade ≥3 infections, 22.2% and 61.5%). CRS was common and limited to grade 1/2.19
Step-up dosing and the impact on CRS and ICANS
The initial step-up regimen in ELM-2 consisted of 1 mg split over days one and two of cycle one and 20 mg split over days eight and nine of cycle one, followed by the 80 mg full dose on day 15 of cycle one (1/20 regimen). The 1/20 regimen was revised during the study to further mitigate CRS risk by adding an intermediary step-up dose. The modified regimen consisted of 0.7 mg split over day one of cycle one (0.2 mg) and day two of cycle two (0.5 mg), 4 mg split over days eight and nine of cycle one, and 20 mg split over days 15 and 16 of cycle one, followed by the 80-mg full dose on day one of cycle two (0.7/4/20 regimen). The treatment showed an acceptable safety profile with 0.7/4/20 step-up dosing compared to the other CD20xCD3 bispecific antibodies. Treatment-emergent adverse events (TEAEs) occurred in 86 (90%), with the most common TEAEs (>30% all grades) being CRS (51%), pyrexia (32%), anemia (31%), and infusion-related reaction (31%). In the R/R DLBCL cohort, the most common TEAEs (>30% all grades) were CRS (55%), anemia (43%), and pyrexia (42%). With the optimized 0.7/4/20 mg step-up regimen, 98% of CRS events were Grade 1/2, and only one Grade 3 CRS (confounded by pancreatitis) was reported. Supportive measures resolved CRS events. No ICANS events were reported with the optimized step-up regimen.12-14
Following implementation of the 0.7/4/20 step-up regimen in C1, no Grade ≥2 CRS was observed; only Grade 1 CRS was reported in 39% of patients. All CRS events resolved and only one patient received tocilizumab for CRS management. No ICANS was reported in the 0.7/4/20 regimen compared with 3% in the 1/20 regimen. Overall, the treatment was well tolerated and may present an important treatment option for patients with R/R FL.8,10,11
Other targeted FDA-approved therapies for the treatment of NHL include:
- Bruton’s tyrosine kinase (BTK) inhibitors: ibrutinib, acalabrutinib, and zanubrutinib4,8
- BCL-2 inhibitor: venetoclax, sonrotoclax4,8,20
- Immunomodulatory drug: lenalidomide4,8
- Histone deacetylase (HDAC) inhibitors: belinostat, and vorinostat4,8
- Proteasome inhibitor: bortezomib1
Bone Marrow Transplant4,6
This involves using high doses of radiation and chemotherapy to suppress the patient’s bone marrow and immune system. Transplants are either autologous (patient’s own stem cells) or allogeneic (donor stem cells).
Further details on each of these therapies can be accessed in the Resources section.
References:
- Paquin AR, Oyogoa E, McMurry HS, Kartika T, West M, Shatzel JJ. The diagnosis and management of suspected lymphoma in general practice. Eur J Hematol. 2023;110:3-13. doi:10.1111/ejh.13863
- Bradstock K, Browett P. Leukaemia & Blood Foundation. Early diagnosis and referral of lymphoma is critical. (https://www.leukaemia.org.nz/assets-prod/downloads/Information-Booklets-SS-Documents/Early_diagnosis_article.pdf).
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 3.2026. March 12, 2026. (https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf).
- American Cancer Society. Treating Non-Hodgkin Lymphoma. (https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/treating.html).
- Mayo Clinic. Non-Hodgkin lymphoma. Diagnosis and Treatment. November 7, 2025. (https://www.mayoclinic.org/diseases-conditions/non-hodgkins-lymphoma/diagnosis-treatment/drc-20375685).
- Tucker D, Thiebaud CM. An overview of the treatment of non-Hodgkin lymphoma with the novel cellular therapies: CAR T and bispecific monoclonal antibodies. Med Res Arch. 2023;11. doi:10.18103/mra.v11i9.4494
- Regeneron. News release. Ordspono™ (odronextamab) Approved in the European Union for the Treatment of Relapsed/Refractory Follicular Lymphoma and Diffuse Large B-cell Lymphoma. August 26, 2024. (https://investor.regeneron.com/news-releases/news-release-details/ordsponotm-odronextamab-approved-european-union-treatment).
- Abou Dalle I, Dulery R, Moukalled N, et al. Bi- and Tri-specific antibodies in non-Hodgkin lymphoma: Current data and perspectives. Blood Cancer J. 2024;14:23. doi:10.1038/s41408-024-00989-w
- Sehn LH, Bartlett NL, Matasar MJ, et al. Long-term 3-year follow-up of mosunetuzumab in relapsed or refractory follicular lymphoma after ≥2 prior therapies. Blood. 2025;145:708-719. doi:10.1182/blood.2024025454
- Radhakrishnan VS, Davies AJ. Bispecific antibodies in indolent B-cell lymphomas. Front Immunol. 2024;14:1295599. doi:10.3389/fimmu.2023.1295599
- Russler-Germain DA. Ghobadi A. T-cell targeting therapies for B-cell non-Hodgkin lymphoma: Recent progress and future directions. Front Oncol. 2023;13:1168622. doi:10.3389/fonc.2023.1168622
- Bannerji R, Arnason JE, Advani RH, et al. Odronextamab, a human CD20×CD3 bispecific antibody in patients with CD20-positive B-cell malignancies (ELM-1): Results from the relapsed or refractory non-Hodgkin lymphoma cohort in a single-arm, multicentre, phase 1 trial. Lancet Haematol. 2022;9:e327-e339. doi:10.1016/S2352-3026(22)00072-2
- Bisneto JV, Jagadeesh D, Stevens, et al. Efficacy and safety of long-term odronextamab treatment in patients with relapsed/refractory follicular lymphoma: 3-year follow-up from the Phase 2 ELM-2 study. ASH 2025 Annual Meeting. Abstract 3588.
- Brem E, Jurczak W, Belada D, et al. 4411 Odronextamab monotherapy in previously untreated patients with high-risk follicular lymphoma (FL): Results of the safety lead-in of the phase 3 Olympia-1 study. Blood. 1442024;144(suppl 1):4411. doi:10.1182/blood-2024-200080
- Wudhikarn K, Hacibekiroglu T, Hernandez Rivas JA, et al. Odronextamab plus chemotherapy in patients with previously untreated follicular lymphoma: First results from part 1 of the Phase 3 Olympia-2 study. Blood. 2025;146(suppl 1):3600. doi:10.1182/blood-2025-3600
- Kim WS, Kim TM, Cho SG, et al. Odronextamab monotherapy in patients with relapsed/refractory diffuse large B cell lymphoma: primary efficacy and safety analysis in phase 2 ELM-2 trial. Nat Cancer. 2025;6:528-539. doi:10.1038/s43018-025-00921-6
- Topp MS, Matasar M, Allan JA, et al. Odronextamab monotherapy in R/R DLBCL after progression with CAR T-cell therapy: Primary analysis of the ELM-1 study. Blood. 2025;145:1498-1509. doi:10.1182/blood.2024027044
- Allan JN, Crombie JL, Matasar M, et al. 3118 Long-term efficacy and safety of odronextamab in relapsed/refractory diffuse large b-cell lymphoma (DLBCL): Pooled analysis from the ELM-1 and ELM-2 studies. Blood. 2024;144 (suppl 1):3118. doi:10.1182/blood-2024-199980
- Michot JM, Yagci M, Kargus K, et al. Odronextamab plus chemotherapy in patients with previously untreated diffuse large B-cell lymphoma (DLBCL): First results from part 1 of the Phase 3 Olympia-3 study. Blood. 2025;146(suppl 1):65. doi:10.1182/blood-2025-65
- US Food and Drug Administration. FDA grants accelerated approval to sonrotoclax for relapsed or refractory mantle cell lymphoma. May 13, 2026. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-sonrotoclax-relapsed-or-refractory-mantle-cell-lymphoma
ALL URLs accessed April 27, 2026
