Diagnosis & Staging
Challenges in Diagnosis
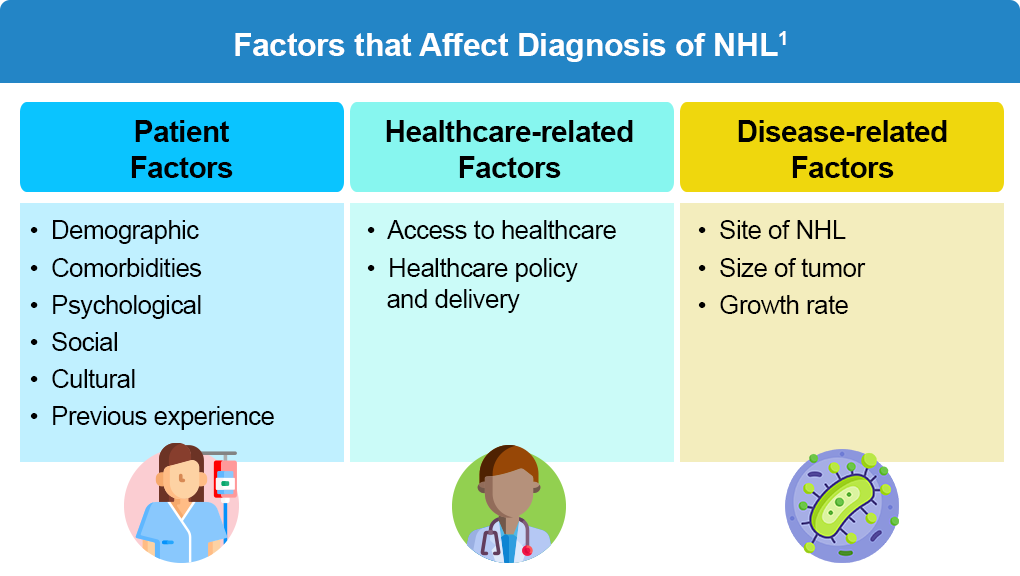
Early diagnosis of NHL is important for improving patient survival and quality of life. However, several factors can delay diagnosis, and there remains limited guidance for primary care physicians after other differential diagnoses have been effectively ruled out and lymphoma has emerged as the most likely diagnosis.1,2
Clinical Presentation
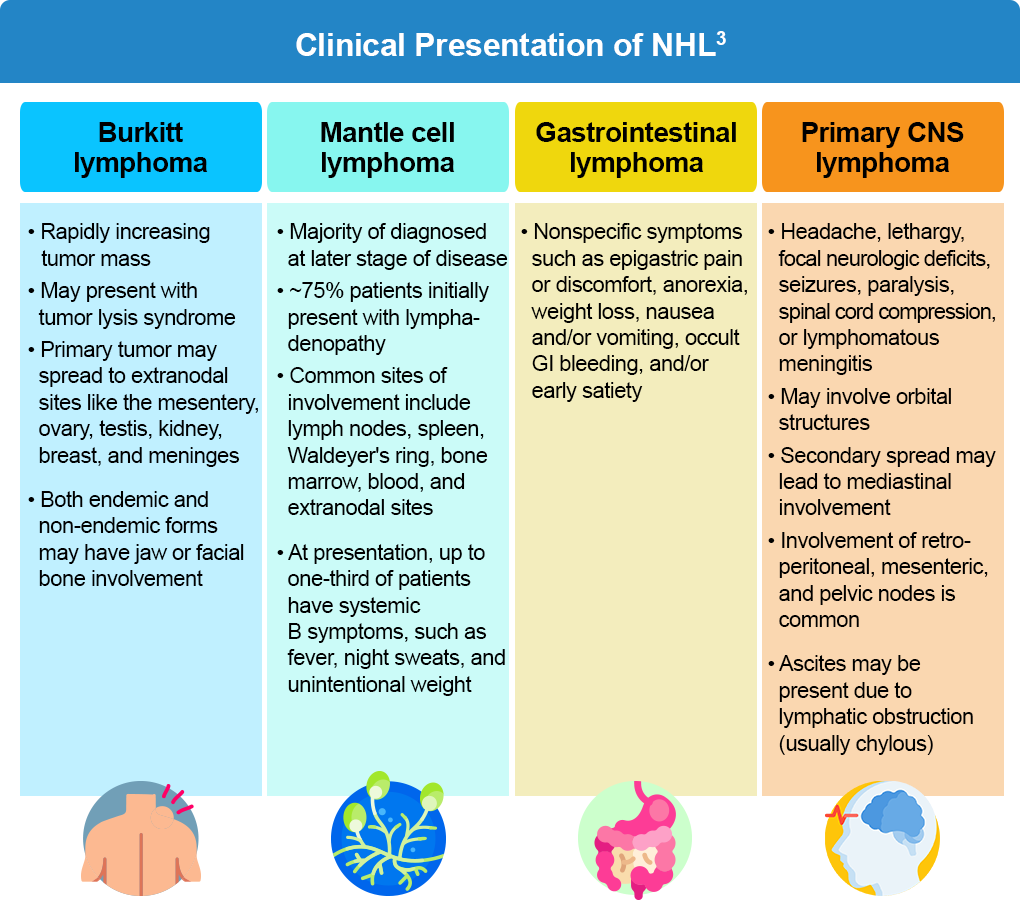
Clinical presentation varies according to the site involved. Clinical features of NHL differentiated by subtype are listed below in the table.3
Diagnosis
The diagnostic workup of lymphoma includes a personal and family history, assessment of symptoms (including B symptoms and peripheral lymphadenopathy), and a physical examination with attention to node-bearing areas as well as liver and spleen size. Additionally, several of the tests listed below may be performed to confirm the diagnosis and assess disease extent and baseline organ function.2-4
- Blood tests may include a complete blood count (CBC) with differential, lactate dehydrogenase (LDH), comprehensive metabolic panel (CMP), pregnancy panel, and beta-2-microglobulin, in addition to infectious disease testing.
- Low hemoglobin levels, along with low red blood cell count, hematocrit, or platelet counts may indicate anemia. A CBC may indicate cytopenia, lymphocytosis, or thrombocytosis, due to extensive bone marrow infiltration, hypersplenism, or blood loss from gastrointestinal tract involvement.2-4
- A CMP may identify tumor lysis syndrome, commonly seen in rapidly proliferative NHL such as Burkitt lymphoma or lymphoblastic lymphoma. LDH levels may be elevated from high tumor burden or extensive infiltration of the liver.
- Beta-2-microglobulin is a measure of disease burden4
- Infectious serology (Hepatitis B, C, and HIV) may indicate a particular subtype5
- Imaging includes PET/CT scan (including neck) with contrast, PET/CT scan and/or chest/abdominal/pelvic CT with contrast of diagnostic quality, abdominal ultrasound, and/or endoscopy/colonoscopy
- Bone marrow studies including bone marrow biopsy + aspirate, histology, cytology, immunophenotyping (IHC panel or cell surface marker analysis by flow cytometry with peripheral blood and/or biopsy specimen)
- Evidence of toxicity assessed by evaluating creatinine clearance, uric acid, ECG/MUGA scan, cardiac ultrasound (before anthracyclines), pulmonary function (ASCT)
- Lumbar puncture is often reserved for those at high risk for CNS involvement (ie, highly aggressive NHL, Burkitt lymphoma, DLBCL, peripheral T-cell lymphoma, grade 3B FL, mantle cell lymphoma, precursor T or B lymphoblastic leukemia/lymphoma, human immunodeficiency virus (HIV)-positive NHL), who have epidural, bone marrow, testicular, or paranasal sinus involvement, or at least two extranodal disease sites. CSF should be sent for both cytology and flow cytometry
- FISH (fluorescence in situ hybridization) is a molecular analysis used to detect extra or missing chromosomes or gene rearrangements in cells and tissues
For all B-cell lymphomas, diagnosis is confirmed via excisional or incisional biopsy; a fine needle aspiration (FNA) biopsy on its own is not considered suitable for initial diagnosis. A combination of core needle biopsy (preferably multiple biopsies) and FNA biopsies in conjunction with other techniques such as immunohistochemistry (IHC), flow cytometry, and molecular analysis for the detection of immunoglobulin, gene rearrangements, karyotype, or FISH for major translocations, may be sufficient for diagnosis. Additionally, hematopathology review of all slides with at least one paraffin block representative of the tumor is required.2 Additional diagnostic tests for each type of NHL may be required; information about these can be found in the Resources section.
Differential Diagnosis
The symptoms of several medical conditions mimic symptoms of non-Hodgkin lymphoma. Clinical presentation may include localized or generalized lymphadenopathy. Flow cytometry and cytogenetics help in the differentiation of various conditions.6
Medical conditions similar to NHL:
- Hodgkin lymphoma
- Epstein Barr virus infection
- Systemic lupus erythematosus
- Intussusception
- Appendicitis
- Toxoplasmosis
- Metastasis from the primary tumor (eg, nasopharyngeal carcinoma, soft tissue sarcoma)
- Malignancies or lymphoproliferative disorders like granulocytic sarcoma and multicentric Castleman disease
- Mycobacterial and other bacterial infections that cause benign lymph node infiltration and reactive follicular hyperplasia
Staging
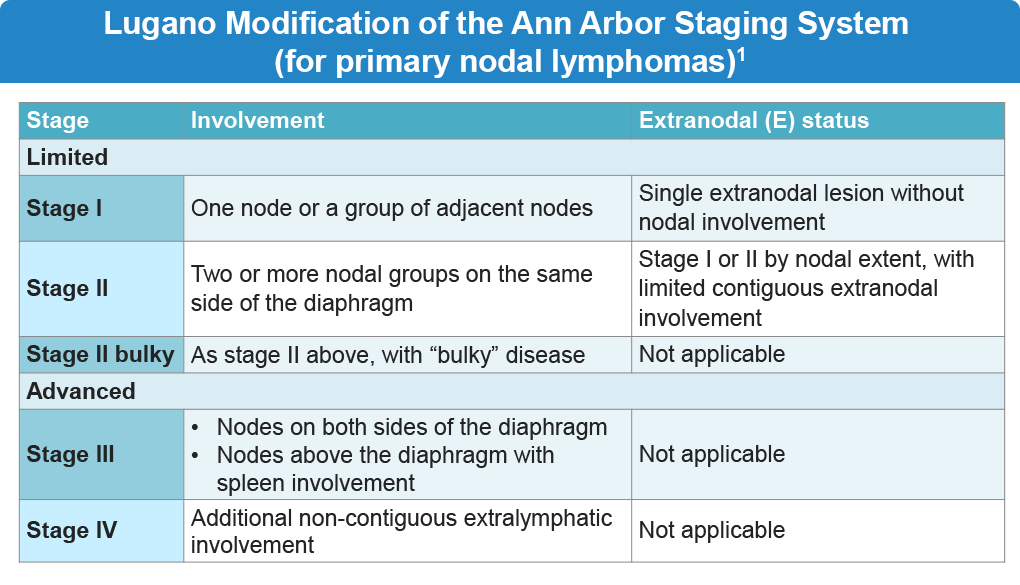
Staging defines the anatomic extent of disease and informs treatment selection.3 Lugano modification of the Ann Arbor system remains the standard system for NHL staging, with notation for bulky disease when present.
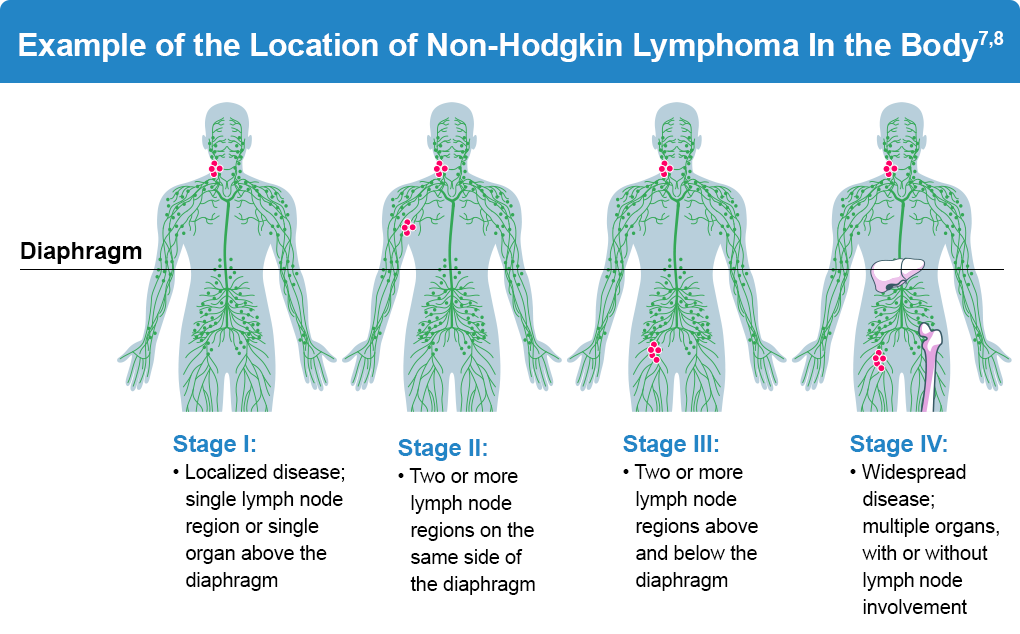
Prognostic indices such as the International Prognostic Index (IPI) are used for NHL risk stratification. For Follicular lymphoma (FL), the FL International Prognostic Index (FLIPI) is used to categorize patients as low (0-1 factor), intermediate (2 factors), or high (3-5 factors) risk. Factors include nodal sites (>4 lymph nodes), age (>60 years), serum marker (elevated LDH), staging (advanced Ann Arbor classification stage III-IV), and hemoglobin (<12 g/dL). For patients requiring treatment, a revised FLIPI2 score incorporating beta-2-microglobulin, diameter of the largest lymph node, bone marrow involvement, and hemoglobin levels is available. An example of NHL staging by extent of disease and lymph node involvement is shown below.3,7
NHL Staging
References:
- Howell DA, Hart RI, Smith AG, Macleod U, Patmore R, Roman E. Disease-related factors affecting timely lymphoma diagnosis: A qualitative study exploring patient experiences. Br J Gen Pract. 2019;69:e134-e145. doi:10.3399/bjgp19X701009
- Paquin AR, Oyogoa E, McMurry HS, Kartika T, West M, Shatzel JJ. The diagnosis and management of suspected lymphoma in general practice. Eur J Hematol. 2023;110:3-13. doi:10.1111/ejh.13863
- Sapkota S, Shaikh H. Non-Hodgkin Lymphoma. StatPearls. Last updated February 24, 2023. (https://www.ncbi.nlm.nih.gov/books/NBK559328/).
- Gupta G, Ghalaut VS, Lokanathan V, Sharma P. 33P Prognostic significance of serum beta 2 microglobulin in non-Hodgkin lymphoma. Ann Oncol. 2017;28(suppl 10):x9. doi:10.1093/annonc/mdx653.010
- American Cancer Society. Tests for Non-Hodgkin Lymphoma. Last revised: February 15, 2024. (https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/detection-diagnosis-staging/how-diagnosed.html).
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: A review. J Family Med Prim Care. 2020;9:1834-1840. doi:10.4103/jfmpc.jfmpc_1037_19
Dreyling M, Ghielmini M, Rule S, et al. Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32:298-308. doi:10.1016/j.annonc.2020.11.008
Blood Cancer United. Non-Hodgkin lymphoma (NHL) diagnosis. (https://bloodcancerunited.org/blood-cancer/lymphoma/non-hodgkin-lymphoma/diagnosis).
ALL URLs accessed April 27, 2026
