Guideline Recommendations
First-line treatment of NHL
First-line treatment for most subtypes of NHL is R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). Other recommended regimens include dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, plus rituximab).1
Diffuse large B-cell lymphoma
The table below shows the recommended front-line treatment options for DLBCL. Presenting symptoms include rapidly enlarging masses with both local and systemic symptoms (B symptoms, such as fever, night sweats, and weight loss).1,2
Most patients with localized tumors can be cured with chemotherapy alone or in combination with immunomodulatory agents. For advanced disease, approximately 60% of the patients are cured by R-CHOP, with improved outcomes using novel regimens like Pola-R-CHP.2

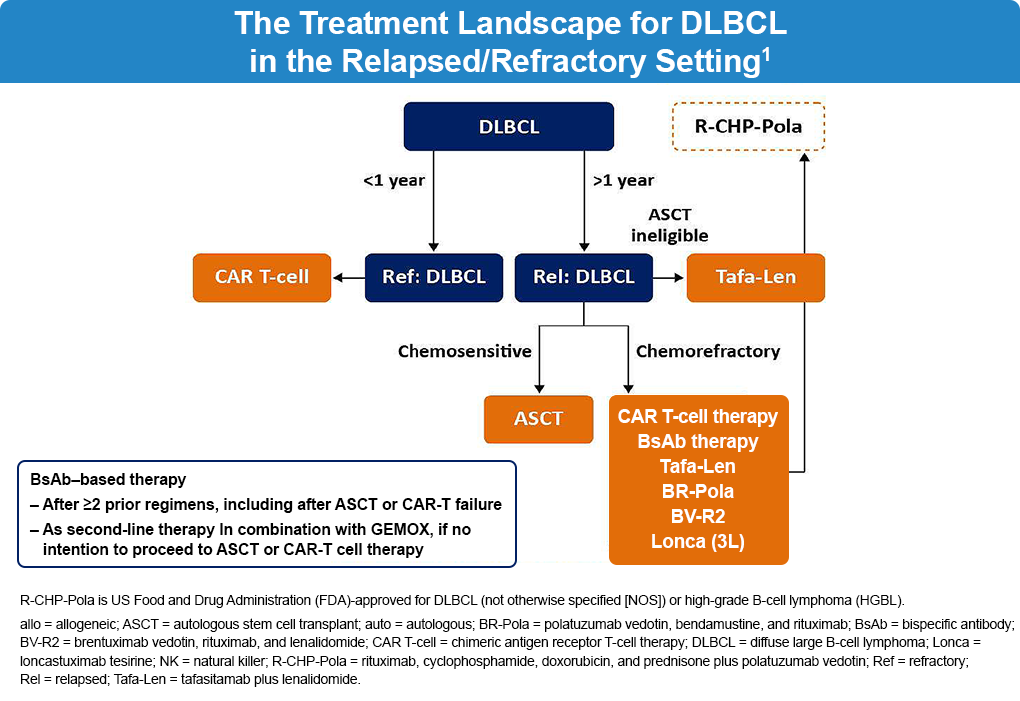
In relapsed/refractory DLBCL, treatment selection is guided by timing of relapse (<12 months vs ≥12 months after front-line therapy), chemosensitivity, and transplant eligibility. Patients with primary refractory disease or relapse within 12 months are typically considered for CAR T-cell therapy, whereas those with later relapse may receive salvage chemoimmunotherapy followed by autologous stem cell transplantation (ASCT). For patients who are not candidates for ASCT or who have chemorefractory disease, additional options include CAR T-cell therapy and novel agents such as tafasitamab plus lenalidomide or antibody-drug conjugates. Importantly, bispecific antibodies have emerged as a key treatment option in relapsed and refractory DLBCL, including in patients who have received ≥2 prior lines of therapy or progressed after CAR T-cell therapy, offering an off-the-shelf immunotherapy approach with demonstrated clinical activity.1
Follicular lymphoma
Follicular lymphoma is a tumor arising from follicle center cells, typically a combination of centrocytes and centroblasts.2 As it is an indolent tumor, median survival ranges from 8-15 years. Watchful waiting and deferment of treatment until the patient has symptoms is an option in patients with advanced FL and remains a standard of care.3 Rituximab alone or in combination with various chemotherapeutic drugs or in combination with immunomodulating agents (eg, lenalidomide) is a first-line treatment.4
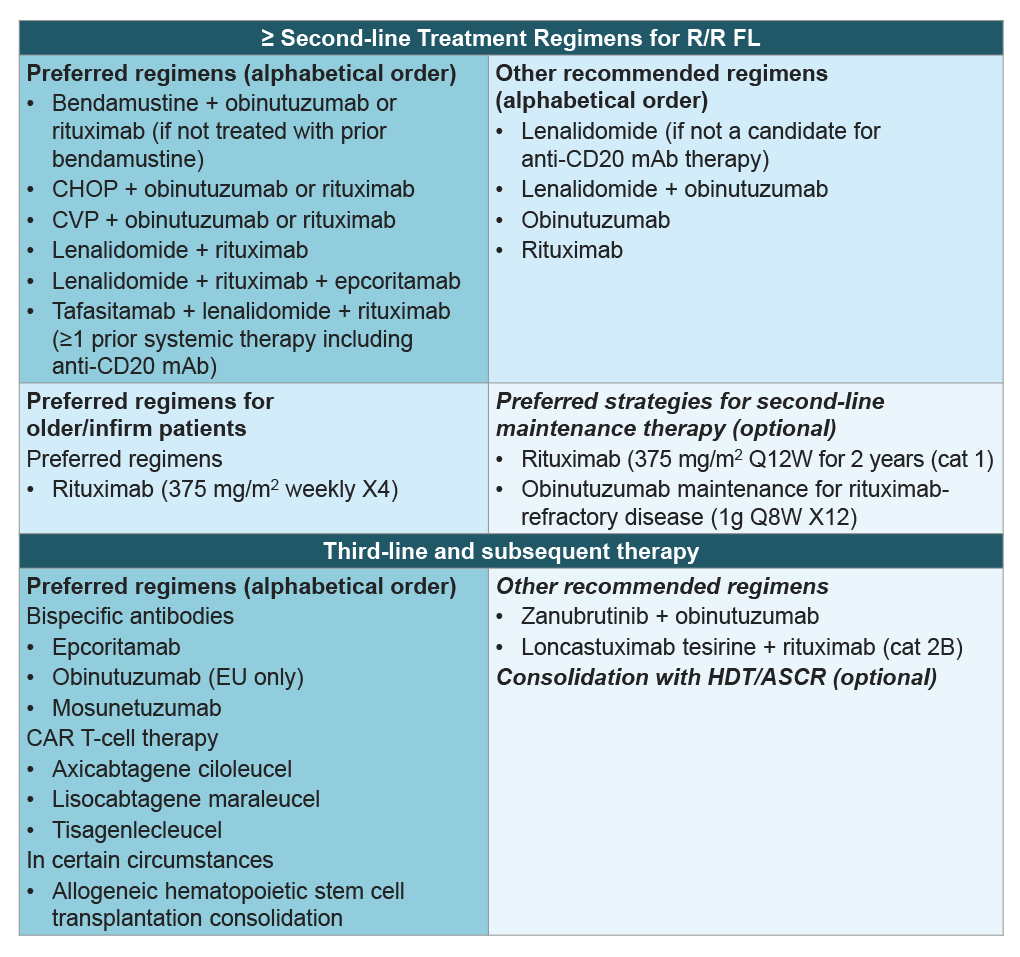
The treatment landscape for R/R FL has changed significantly during the last few years, with several novel agents now available. Recommended regimens for second-line therapy include anti-CD20 mAB-based regimens as well as the CD19-targeted mAB, tafasitamab, in combination with lenalidomide. In the third-line setting, novel immunotherapy options, including CD20xCD3 bispecific antibodies and CD19-targeted CAR-T cell therapies are preferred. Additional recommended options include zanubrutinib + obinutuzumab and the anti-CD19 antibody-drug conjugate, loncastuximab tesirine with rituximab. Autologous or allogeneic stem cell transplants may also be considered as consolidation therapy for relapsed disease. The table below outlines various therapeutic options for R/R FL.1
Patients with indolent lymphomas may develop a more aggressive histology upon relapse, and a biopsy at this stage can help inform an appropriate change to the therapy to match that histologic subtype.1
Mantle cell lymphoma
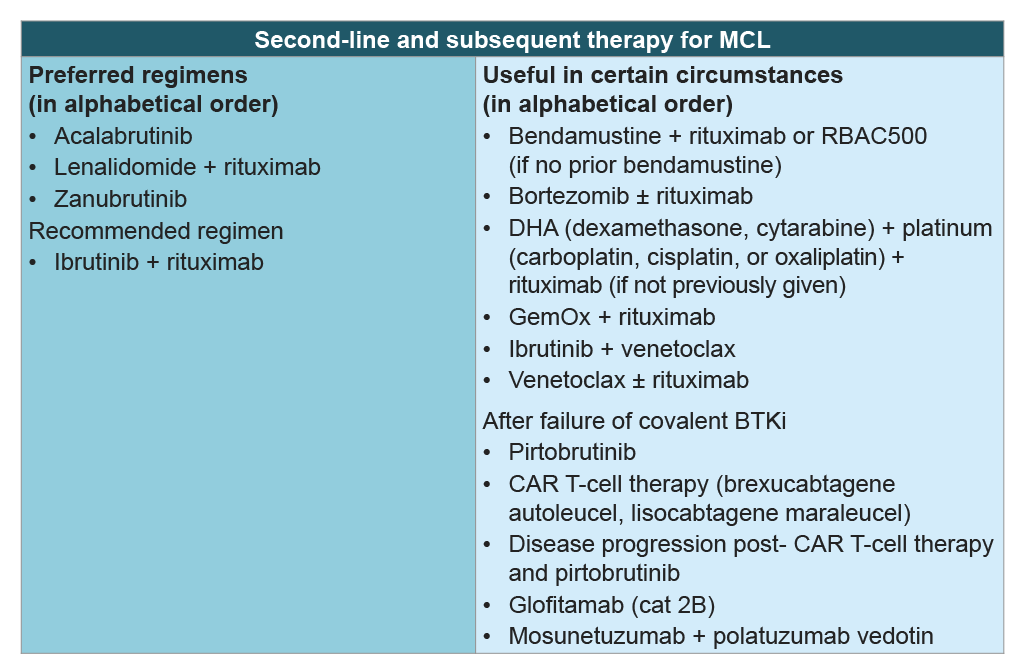
MCL is a heterogeneous subtype of B-cell NHL. It is difficult to treat mantle cell lymphoma with conventional chemoimmunotherapy as it has the unfavorable characteristics of both indolent and aggressive NHL, along with a typically more aggressive disease course compared to indolent NHL. The standard treatment regimen for induction therapy is not yet established. There are no prospective randomized studies comparing the various aggressive regimens or for the addition of a BTK inhibitor to the chemoimmunotherapy regimens. The table below illustrates treatment options for R/R MCL.1
References
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. B-Cell Lymphomas. Version 3.2026. March 12, 2026. (https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf).
- PDQ Adult Treatment Editorial Board. Adult Non-Hodgkin Lymphoma Treatment (PDQ®): Health Professional Version. In: PDQ Cancer Information Summaries. National Cancer Institute. May 18, 2023. (https://www.ncbi.nlm.nih.gov/books/NBK66057/).
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: A review. J Family Med Prim Care. 2020;9:1834-1840. doi:10.4103/jfmpc.jfmpc_1037_19
- Armitage JO, Longo DL. Is watch and wait still acceptable for patients with low-grade follicular lymphoma? Blood. 2016;127:2804-2808. doi:10.1182/blood-2015-11-632745
ALL URLs accessed April 27, 2026
